



LA Times (12/15/20) reports that Pfizer vaccine is “74.4% effective in Asian Americans, and…only 10.4% effective” among people described as multiracial—though in both cases, only one vaccinated person in the demographic came down with Covid.
Science reporting frequently fails to meaningfully communicate research results, especially when it comes to medical research. Out of context numbers and percentages only create public misunderstanding of the scientific results.
When the LA Times (12/15/20) published Karen Kaplan’s comparison of the Moderna and Pfizer Covid-19 vaccines consisting essentially of a list of percentages without explanation, it created the impression that one vaccine was better than the other for certain populations. Asian parents sent the article to their children urging them to get the Moderna vaccine if possible. Yet these numbers were calculated with a sample size too low to make even a guess of that conclusion.
Many people have seen in numerous news stories and press releases that both of these vaccines have about 95% efficacy. But news stories don’t explain how these numbers are calculated. Vaccine efficacy (VE) is calculated by comparing the difference in rate of infection between the vaccinated group and the placebo group.
The efficacy calculation used in these vaccine trials is reduction in relative risk in the vaccinated group, calculated with this formula:

In the Moderna vaccine trial, 13,934 study participants received the vaccine and five of those participants developed Covid-19. 13, 883 participants received the placebo and 90 of those participants developed Covid-19. (Source: Page 23, Table 9 of FDA Moderna briefing document)
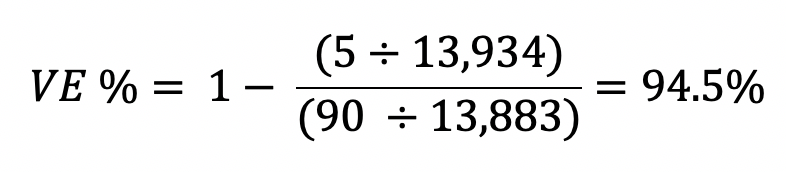
In the Pfizer vaccine trial, 18,198 study participants received the vaccine and eight of those participants developed Covid-19. 18,325 participants received the placebo and 162 of those participants developed Covid-19. (Source: Page 24, Table 6 of FDA Pfizer briefing document)

These numbers answer the question the LA Times poses, “How effective are the vaccines overall?” The FDA had signaled it was prepared to consider emergency use authorization to any vaccine with over 50% efficacy, and these VE percentages were well above that threshold.
But then, the LA Times article goes on to ask the same question for different populations, and answers it based on the VE % for different subgroups published in the study data. The problem is that many of these subgroups do not have a large enough sample size of study participants who developed Covid-19 for this VE % to be statistically evaluable.
The data are displayed in the documents for completeness, but any difference between the subgroup VE % and the overall VE % is most likely due to chance. Publishing these numbers as if the Pfizer vaccine is 100% effective in Pacific Islanders when there was only one case of Covid-19 among Pasifika participants for the analysis is irresponsible and misleading.
Calculations for how each VE % published in the LA Times article are shown in the following table, and show how absurd it is to conclude that one vaccine is better than the other for any of these subgroups. The comparisons made were not always even between subgroups of the same criteria, for example showing the VE % for ages 65+ for the Moderna trial and ages 56+ for the Pfizer trial in the evaluation of whether these vaccines are effective in older people.
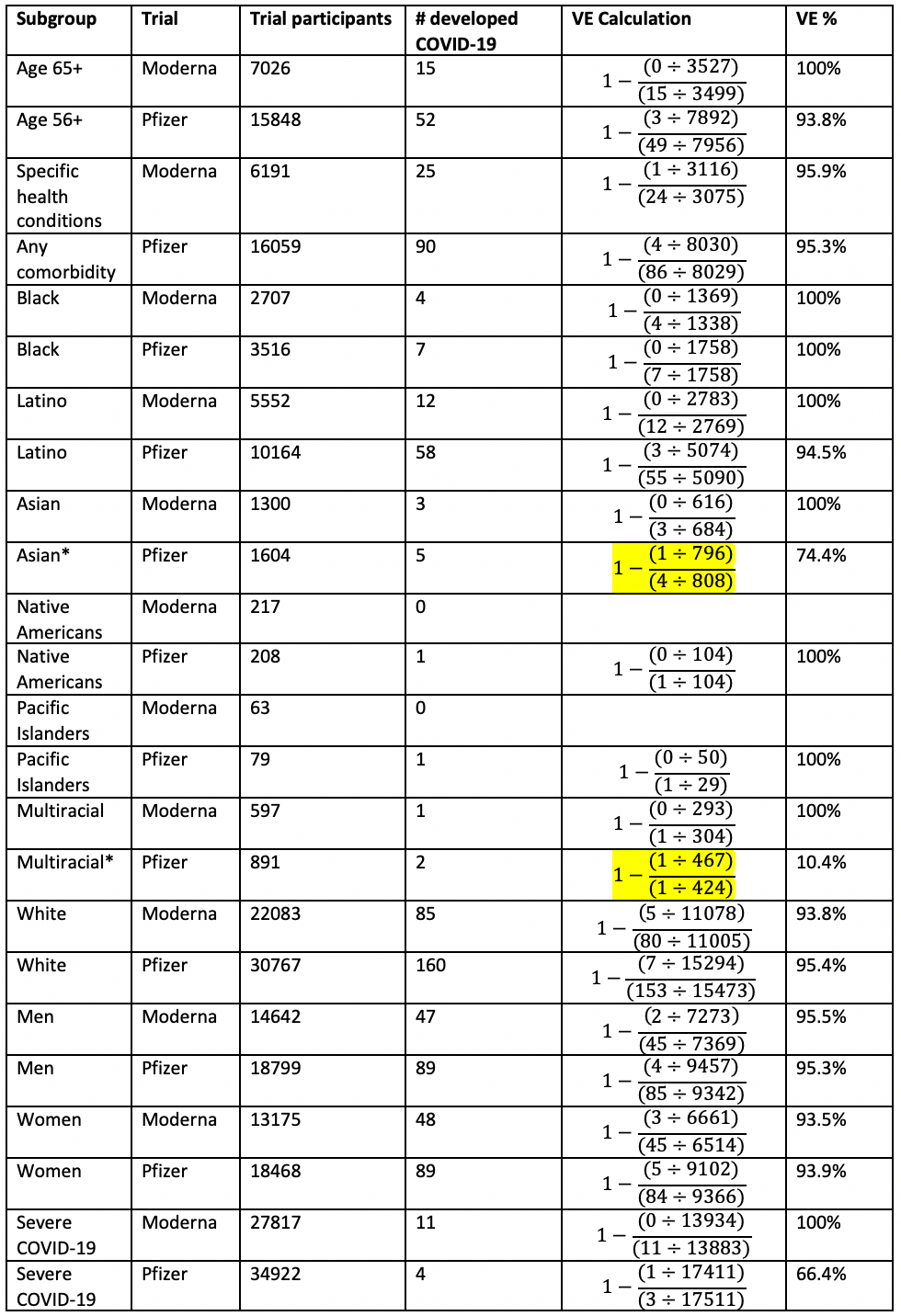
Note: We calculated Pfizer’s Asian and Multiracial VE% to be 74.6% and 10.9%, respectively, but they appear as 74.4% and 10.4%, respectively, in Pfizer’s FDA briefing.
There simply is not enough data to assess efficacy among groups that make up a small percentage of the trial participants. While there are efforts to recruit people of color and older trial participants, and most of these trials end enrollment for younger white people once they reach certain overall enrollment goals, it would take thousands more Asian, Black and other trial participants to make any meaningful assessment on the vaccine’s efficacy for any of these specific groups.
Overblown racial disparity

Yahoo! (12/4/20) says a vaccine simulation “examine[s] a vaccine similar to these big developers'”–but they differ in precisely the way the study found to be problematic.
Likewise, the reporting on the MIT machine learning study, as in a Yahoo! report (12/4/20), wrongly implies that the Pfizer and Moderna vaccines may not be as effective for Asian and Black participants:
Researchers used artificial intelligence and machine learning to examine a vaccine similar to these big developers’, and found that while less than 0.5% of white trial participants didn’t respond strongly to the vaccine, nearly 10% of Asian participants didn’t.
This is misleading, and overblows the potential racial disparity in vaccine efficacy. For a summary of the immunological reasons for this, please refer to this Twitter thread by professor of immunology Akiko Wasaki. Yahoo! also reports on the study as if it were a clinical trial performed on real people, but it was a computer simulation that modeled theoretical vaccines.
The MIT study found striking simulated racial disparities for a predicted vaccine that only encodes the receptor binding domain (RBD) of the spike protein: 37.3% of Asian people’s immune systems wouldn’t be able to recognize an RBD vaccine.
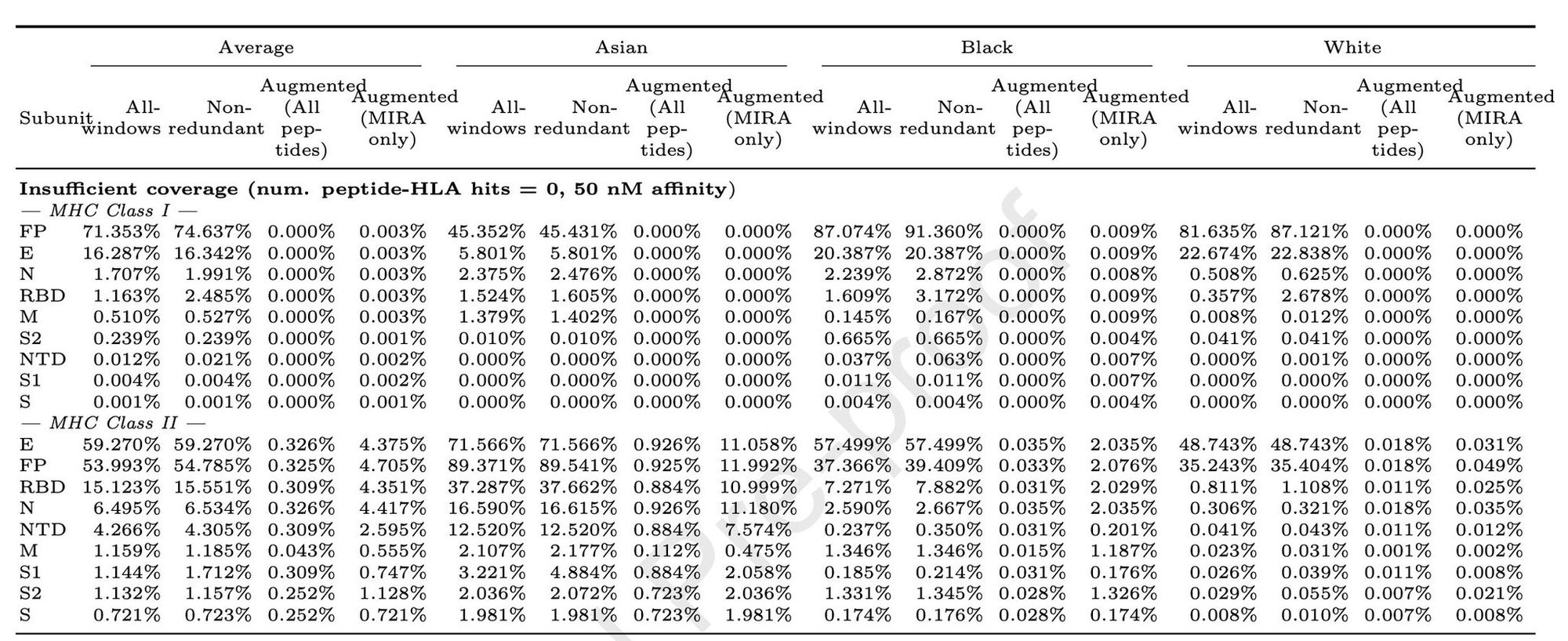
For whole spike protein vaccines (S), >99% of all people’s MHC class I can present at least 1 peptide, and >98% of Asian people’s MHC class II can present at least 1 peptide.
However, Moderna’s vaccine encodes the entire spike protein. Astrazeneca’s vaccine encodes the entire spike protein. Pfizer performed trials on two vaccine variants: one encoding only the RBD and one with whole spike protein. The whole spike protein version of Pfizer’s vaccine is the only one approved for emergency use in the UK and US. The MIT study actually predicts more than 98% robust coverage for every demographic group for a vaccine that encodes the whole spike protein.
The study does say that vaccines which contain the whole virus, or at least includes more than one viral protein, are more robustly effective than a vaccine which only expresses the spike protein. For example, we can infer from the MIT study that SinoVac’s inactivated virus vaccine may be more effective than any vaccines developed by Operation Warp Speed. However, the MIT study suggests that all the vaccines developed by these US companies are predicted to be effective for most people in every demographic group as well.
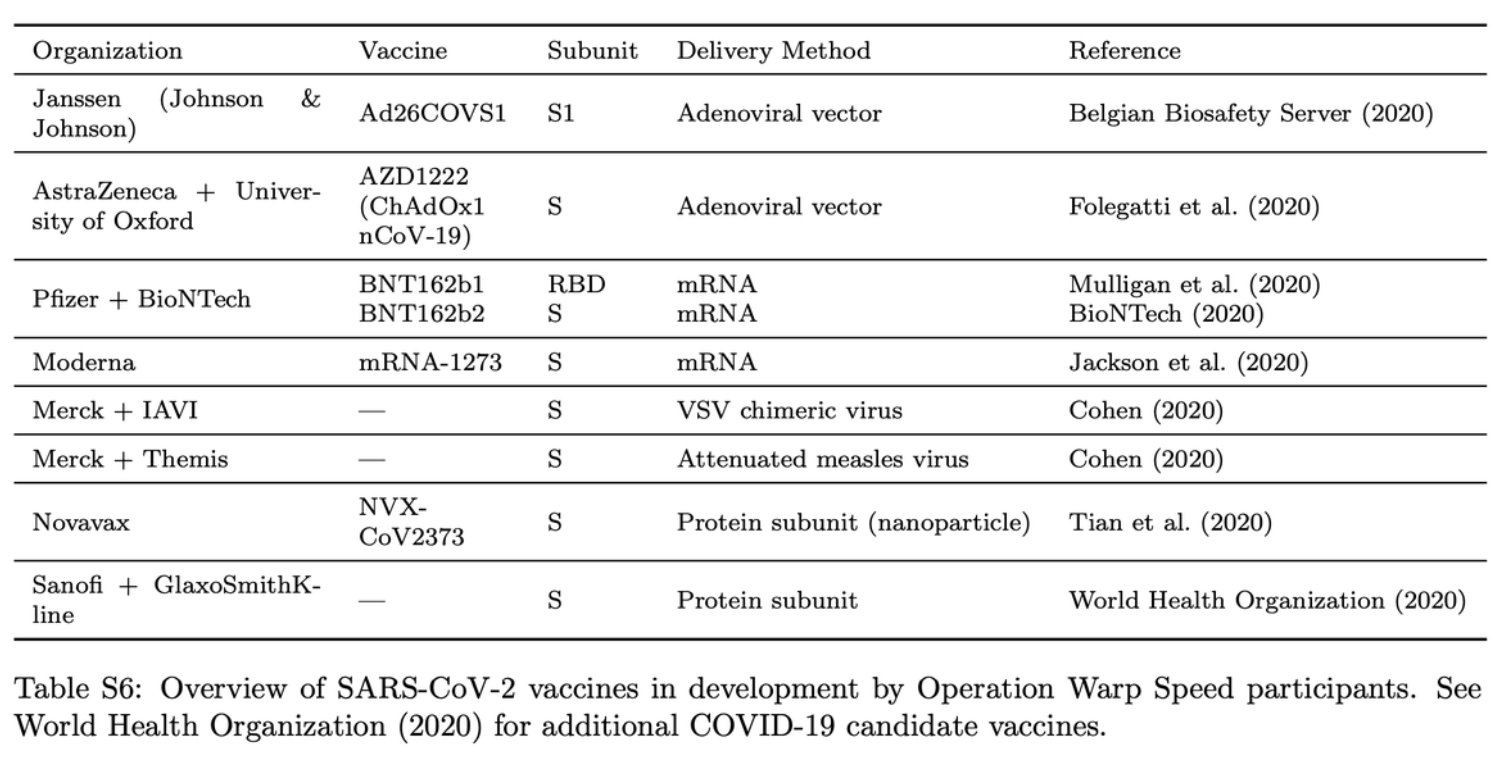
All vaccines in development in the U.S. Operation Warp Speed program. S = whole spike protein; RBD = receptor binding domain of spike protein. Liu et al.
Misleading and distracting
There are two take-home messages we’d like to focus on.
1. Much of the scientific journalism on US Covid vaccines has been inaccurate, misleading, fearmongering and irresponsible. That should make people think extra hard about how poorly represented the Chinese (and likely other future non-Western) vaccines are in any reporting on them done by Western corporate media.
2. The US clearly has enough problems to worry about with domestic Covid containment, vaccine production and distribution, and lack of clear and accurate reporting of information to the people. US corporate media should stop wasting its time speculating on China’s vaccines and Covid caseload from last winter. These are racist distractions that only hurt Americans further.
A version of this article originally appeared in Plan A (12/30/20).

Corpress reporting
More of a dark art than a science
Leading Virologist Says Coronavirus Pandemic is “The Greatest Hoax Ever Perpetrated on an Unsuspecting Public” https://www.wakingtimes.com/leading-virologist-says-coronavirus-pandemic-is-the-greatest-hoax-ever-perpetrated-on-an-unsuspecting-public/ via @wakingtimes
I tried to reply to you “Lloyd”
“Waking Times” is considered to be a conspiracy website pushing quackery.
Check for yourself homie: Media Bias FactCheck has “Waking Times” at the far end of the scale, as both “High” in conspiracy laden material, and “Quackery” (nonsense).
The calculation shown for ‘Relative Risk’ provides the wildly inflated ‘efficacy’ values for these products.
When Absolute Risk is calculated, i.e.; Risk of vaccinated group minus risk of vaccinated group the benefit of vaccination is seen to be < 1%.
Hardly a mandate!
Risk of what, though?
If you’re talking about risk of death, you may be right. But there are other unpleasant effects of COVID besides death.
The metric tracked is “fraction of people in the study who contracted COVID-19 *during the study period.*” This has no real-world corolary, and so the absolute risk cannot be used for any meaningful analysis. The relative risk, expressed here as efficacy, can be usefully interpreted whether or not the absolute risk *in the population* is known.
Absolute risk is useful when discussing risk in a population, or in specific circumstances (e.g. “absolute risk of contracting COVID-19 during your lifetime” or “absolute risk of contracting COVID-19 from attending a gathering of 100 random people without social distancing or masks”). In the case of COVID-19, the absolute risk of someone contracting COVID-19 at some point seems to be extremely high, perhaps greater than 50%. A 95% efficacy reduces this absolute risk to around 2%.
Seems like a clear mandate.
The problem with small, and indeed varying, subgroup sizes is not the total number of participants but the use of single point estimates to report on the results. For instance, there were 74.4% fewer asians who contracted COVID-19 after receiving the Pfizer vaccine. This is largely useless information though, as it is not the same as saying that 74.4% fewer asians in the general population will contract COVID-19 after taking the Pfizer vaccine.
Inferring from the trials to the general population necessarily involves some uncertainty, and the reporting should reflect that uncertainty, rather than attempt to falsely portray a definitive point prediction.
The real estimate for how many fewer asians might contract COVID-19 after receiving the Pfizer vaccine is not 74.4%, but rather between 48% and 98%. In contrast, the efficacy for whites with the Pfizer vaccine may be estimated in the much narrower range of between 92% and 98%. The two estimates completely overlap, so we cannot tell if there is a racially-based difference in efficacy. The difference in the width of these two ranges is entirely due the number of participants in each subgroup; there were far more whites than asians.
Your statement that “there simply is not enough data to assess efficacy among groups that make up a small percentage of the trial participants” is itself misleading. There is enough data; the range of possible real-world values is just quite broad. To your point, the range of possible values with these subgroups is broad enough that we cannot determine a difference between them.
Fantastic article! Very helpful.
However, there’s one glaring omission at the end, when talking about the speculation surrounding Chinese vaccines. It should be noted that the study doesn’t even want to *look* at comparing the Russian vaccine. And there’s a good reason for that. By all accounts, it’s just as effective, but has far fewer side effects. This comes out if you dig deep enough, but you’ll find scarcely a word about it in US media. After trashing the Russian vaccine at first, now that it appears to be superior to Western vaccines, they’re simply trying to pretend it doesn’t exist.
Obviously it can’t be made available to the US public. Because Pharma has to make its money. And because Russophobia is pervasive. So pervasive, so ingrained in our consciousness, that we don’t even recognize it as a bias. Not even an organization like FAIR.
It would be interesting to study the difference in allergic reaction rates and patient mortality between ALL COVID-19 vaccines, including those from Russia and China. It’s also important to look at the practicality and cost of providing those vaccines to people in poor countries. I have a feeling the for-profit US vaccines would not stack up well.
William Thompson proved vaccine injury is worse for POC, but he’s the one whistleblower the Left ignores. It’s incredible, Project Censored acknowledges vaccine injury and Big Pharma perfidy, and FAIR promotes Project Censored, but denies vaccine injury.
Vaccine injury denial works exactly like global warming denial, only instead of being peddled by far-right cynics, it’s pushed by centrists and, oddly, leftists. Even a casual glance at Big Pharma’s complete immunity from tort regarding vaccine safety concerns–the only industry other than the nuclear energy industry that has this bizarre protection–shows why any self-respecting socialist should be highly skeptical of what an industry with no ability to ever be sued, whose damages are paid out by a bizarre “vaccine court” run by the government and paid for with tax dollars, a government which actually owns vaccine patents, thus creating a financial conflict of interest with the industry the government is supposed to be regulating. If the government owned patents on fossil fuel mixtures, the EPA would deny global warming.
The revolving door between Big Pharma and the CDC is as repulsive as the revolving door between the CIA and the world of corporate espionage, but doesn’t get discussed.
Hello Quizzelle,
What may appear to be censorship could be a misunderstanding instead.
William Thompson didn’t “prove” anything. You have to realize, in science there is no such thing as “proof”, there is only evidence and theory. You may be surprised to know this, but science has zero proof the brain causes consciousness. As far as science can tell, the two are only correlated, they have no “proof” that one “causes” the other.
The small trend William Thompson found in autistic children of color, was not to be interpreted as equal in effect over the population at large.
Here is a statement of Abstract about MMR and autism, on a paper coauthored by William Thompson:
“An hypothesis published in 1998 suggested that measles-mumps-rubella vaccine may cause autism as a result of persistent measles virus infection of the gastrointestinal tract. Results of early studies were not supportive and in 2001 a review by the Institute of Medicine concluded that the evidence favors the rejection of a causal relationship at the population level between measles-mumps-rubella vaccine and autistic spectrum disorder. Studies published since the Institute of Medicine report have continued not to find an increased risk of autistic spectrum disorder associated with measles-mumps-rubella. The vaccine also has not been found to be associated with a unique syndrome of developmental regression and gastrointestinal disorders. The evidence now is convincing that the measles-mumps-rubella vaccine does not cause autism or any particular subtypes of autistic spectrum disorder.”
The phrase “at the population level” rules out the small findings in a subgroup that Thompson discovered.
It’s like saying this: Say we were testing a serum for rash, so we tested ten kids: three were white, three were Asian and three were black. We noticed that only two of the black kids had a positive reaction to our serum. Does this mean ALL black people should be assumed to have a positive reaction? Of course not.
Not sure if you read the FAIR article above? The point of the article though, is to NOT equate a tiny statistical finding (based on the group size of POC in the study) to being direct evidence of a trend in the population at large…this is not how the medical research process works (thankfully).
In order to have EVIDENCE (no such thing as proof) of a causal link between harm from vaccinations being higher in populations of people of color, a study would have to be conducted, under controlled laboratory conditions to search for this trend.
How the medical research establishment could set up such a study, without appearing to be harming POC –your guess is as good as mine.
Maybe I’m wrong and I’m the one misreading the story, I don’t know….?
Peace